
Michael Palmer, MD and Sucharit Bhakdi, MD
In the context of the COVID-19 “pandemic”, many people have come to understand that political and scientific authorities have been systematically lying about the origin of the infectious agent, as well as the need for and the safety of mandatory countermeasures, including lock-downs, masks and vaccines. Some skeptics have gone further and begun to question the existence of the virus responsible for COVID-19, or even of viruses and pathogenic germs altogether. Here, we put these questions in perspective.
Before we go into any specifics on germs and viruses, we should acknowledge that the public has ample reason to mistrust not only politicians, public officials and the media, but also the “scientific community.” Even before the COVID-19 pandemic, several very senior members of that community had drawn attention to the deplorable state of scientific integrity in medical research. Particularly poignant is this quote by a former editor-in-chief of one of the world’s leading medical journals, Marcia Agnell [1]:
It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as editor of The New England Journal of Medicine.
Agnell’s assessment is echoed by The Lancet’s editor Richard Horton [1], leading epidemiologist John Ioannidis [2], and Bruce Charlton, former editor of Medical Hypotheses [3]. And, to be sure, this already precarious state declined even further in the COVID-19 “pandemic.” Here are some of the lies regarding COVID-19 that were told alike by politicians and their scientific court jesters the world over:
- the SARS-CoV-2 virus is of natural origin and jumped spontaneously from bats or pangolins to humans;
- PCR-testing of asymptomatic patients is an appropriate means for tracking the spread of COVID-19;
- the early COVID-19 waves threatened to overload the healthcare system to such a degree that it became necessary to destroy the economy in order to “flatten the curve”;
- general vaccination was necessary to overcome the pandemic;
- even though the vaccines were “safe and effective”, vaccinated persons were still at risk of being infected by unvaccinated individuals (but not by other vaccinated ones).
These absurd and brazen lies have been dealt with elsewhere, for example by cardiologist Dr. Thomas Binder [4]. We only cite them here to make it clear that we sympathize in principle with the radically skeptical attitude of much of the public. Nevertheless, we think that in some cases this radical skepticism has been taken too far, and that the proverbial baby has been thrown out with the bathwater. To support our case, we will survey some of the history of “germ theory” of infectious disease.
1. The rise of germ theory in the 19thcentury
The idea that microbes cause transmissible diseases gained acceptance in the late 19thcentury. Its greatest pioneer was Robert Koch, a Prussian physician, who discovered the bacterial agents that cause anthrax, cholera, and tuberculosis. These discoveries paved the way for the prevention of such diseases by hygiene and surveillance.
Even before Koch’s discoveries, Hungarian physician Ignaz Semmelweis had discovered that physicians could avoid transmitting puerperal sepsis from deceased to living mothers through antiseptic hand-washing; but because his empirical procedure lacked a theoretical foundation, it was ultimately abandoned, in spite of its demonstrable success. Semmelweis himself was committed to a psychiatric hospital, where he suffered physical abuse and died shortly after.1
Semmelweis’s personal fate illustrates that the public and the medical community at the time certainly were not ready for “germ theory”, i.e. for the idea of diseases being caused by tangible germs that could be transmitted from one person to the other, but which could also be identified and combated. It therefore is remarkable that Koch’s discoveries were recognized and accepted within a fairly short period of time. Soon, other researchers joined the hunt for further pathogenic bacteria. Other kinds of pathogens soon followed; for example, in 1898 British physician Ronald Ross discovered that the parasite which causes malaria multiplies within and is transmitted by Anopheles mosquitoes.
What brought about this rapid triumph of germ theory? It seems fair to say that both the scientists involved and their audience made it happen. Robert Koch himself was an ingenious and meticulous experimentalist. He set himself an exacting standard for demonstrating that a certain infectious disease was caused by a specific microbe, the well-known “Koch’s postulates” [5]:
- The given organism must be found regularly in the diseased tissue of the infected person or animal.
- The organisms must be capable of being grown in pure culture in the laboratory.
- The pure culture must produce the disease when administered to experimental animals.
- The organisms must be found in the experimentally produced disease, and be capable of being recovered again in pure culture.
While Koch’s comprehensive evidence surely was compelling, his rapid success would not have been possible without his audience. Even though initially skeptical, this audience was also well-educated and open-minded—it had not yet become jaded, cynical, and disoriented by being relentlessly attacked with fake news and junk science.
The great scientists of the 19thcentury were very often hobbyists who were indulging their own whims and passions. They thus were independent from external interests, particularly from financial ones. Academic researchers, too, were more shielded from outside interests than are the “big shots” of today’s institutionalized science. But over the course of the 20thcentury, scientific research institutions became more and more dependent on external funding, often controlled by powerful special interests. This has severely compromised and undermined scientific integrity. We can but wonder, what would Robert Koch think of the likes of Christian Drosten and Tony Fauci? What of the Berlin “public health” institute that bears his name?
2. Successful applications of germ theory
If a theory can be used successfully in practice, this suggests that it is true, or at least a good approximation of the truth. Germ theory has many useful applications; here, we will only give a few early examples for illustration.
Less than a decade after Koch’s discovery of the anthrax bacillus, Friedrich Klein isolated Streptococcus pyogenes, the bacterium which causes puerperal fever, scarlet fever, and various kinds of skin infections. This discovery could explain the earlier success of Semmelweis’s empirically developed hand disinfection procedures for preventing puerperal fever. Hygiene, surveillance and improvements to sanitation made it possible to prevent outbreaks of enteric diseases such as cholera. The city of Hamburg, which initially refused to adopt such precautions, promptly suffered an outbreak of cholera in 1882 that claimed several thousand lives [6]. Robert Koch himself was tasked with overseeing the introduction of hygienic countermeasures, which swiftly brought the outbreak under control.
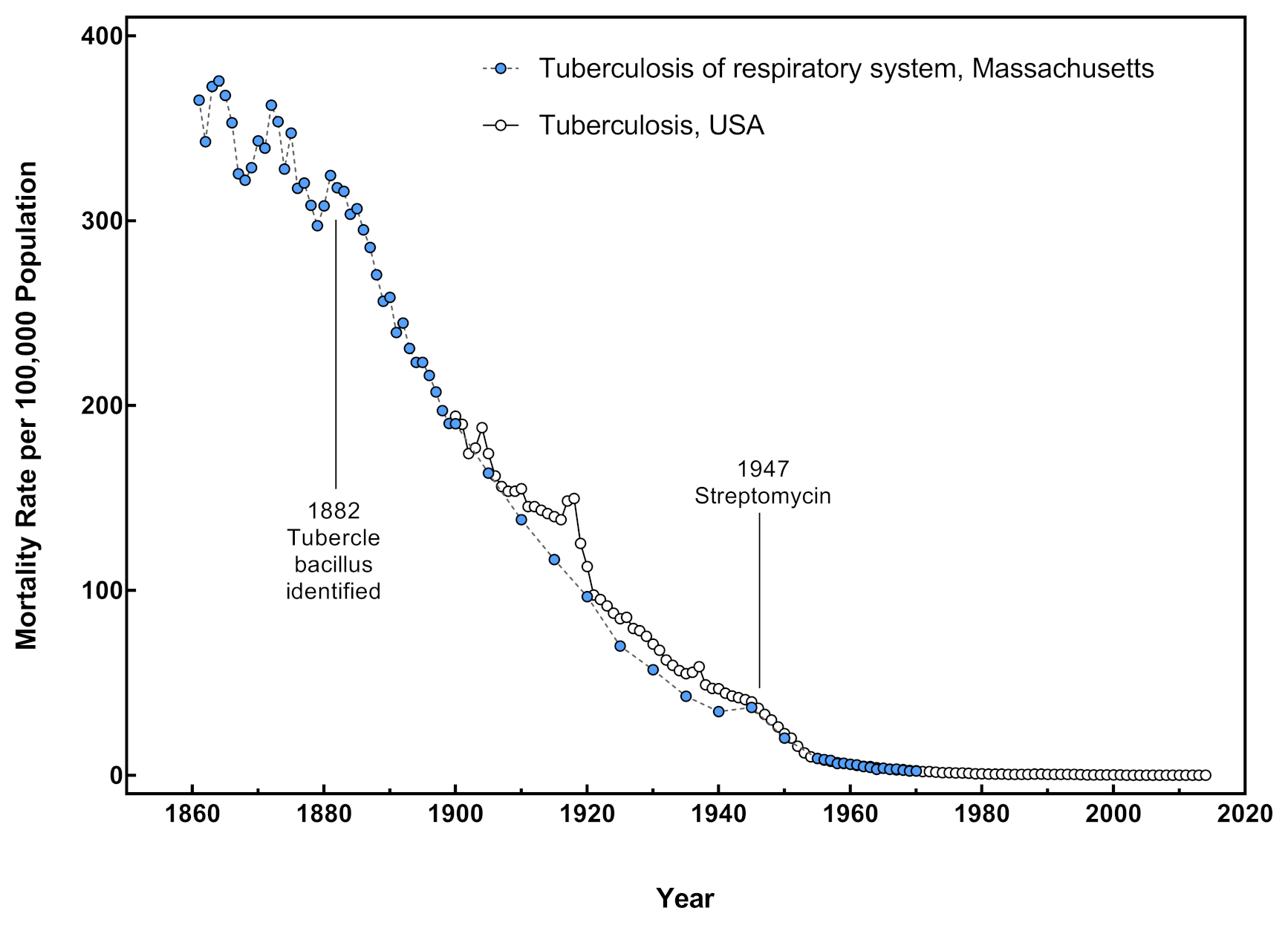
It was mainly through such preventive measures that infectious diseases were conquered, even before specific treatments of manifest infections became available. This is illustrated for tuberculosis in Figure 1. Malcolm Watson, a physician in the colonial service of the British Empire, devised successful methods for controlling malaria. His work, begun only a few short years after Ross had discovered that the malaria parasite was spread by Anopheles mosquitoes, was mostly based on thorough and meticulous drainage of wetlands and regulation of brooks and streams, with quinine prophylaxis and treatment of infections playing only a secondary role [7].
3. Germ theory vs. “terrain theory”—a false dichotomy
Opponents of germ theory like to point to the decisive role of the patient’s general health in susceptibility to infectious disease. This tenet is in fact accepted by mainstream medicine. For example, the significance of age and general health in the prognosis of pneumonia was summed up by the famous Canadian physician William Osler as follows:
Osler’s words, written in 1892, are still true today, largely regardless of the germ in question. It matters not whether the pneumonia be caused by pneumococci, influenza virus, or SARS-CoV-2. Generally speaking, the notion of “opportunistic” infections that befall those in poor general health and states of immunosuppression can be found in the textbooks of medicine. But on the other hand, without any of those opportunistic pathogens, even susceptible individuals would not contract an infectious disease.
Figure 1 shows how, immediately after Koch’s discovery of the tubercle bacillus, mortality due to tuberculosis went into a steep and sustained decline. Most likely, both hygiene and improvements to nutrition and general health contributed to this change for the better. Note, however, that there is no detectable reversal of this trend in the 1930s, i.e. during the Great Depression. In this era, many people were suddenly thrown into poverty, which would most likely also have lowered the quality of their nutrition and their resistance to tuberculosis. The continued decline in tuberculosis mortality in those years was most likely due to the continued surveillance measures.
4. Not all infectious pathogens can satisfy Koch’s postulates
One reads now and then that some pathogenic virus or other microbe does not satisfy Koch’s postulates, which is then construed as proof that it does not cause the disease for which it is known. This is fallacious. Koch’s postulates do not constitute some sort mathematical axiom; they should be understood in their historical context.
Koch needed to convince a public that was initially radically skeptical; thus, the more comprehensive and rigorous his evidence, the easier it would be for him to succeed. It thus made perfect sense for him to focus on pathogens that could be grown in pure culture—that is, in the absence of any other living things—and which could then be inoculated into experimental animals and isolated again as many times as desired. However, once the idea of infectious pathogens had taken hold in principle, it soon became apparent that not all of them met every single postulate in the canon. For example, Rickettsia prowazekii and Treponema pallidum—the bacterial agents that cause typhus or syphilis, respectively—cannot be grown in pure culture, and therefore cannot meet the second, third and fourth postulate. They can, however, be propagated in experimental animals, and Rickettsia prowazekii also in cell culture.
Viruses, by their very nature, can only multiply within living cells but not in pure culture. Therefore, no virus can possibly satisfy Koch’s postulates. However, we repeat that these postulates are not a logical necessity. If they are not fulfilled, the question of disease causation must be settled in some other manner.
5. What does it mean to isolate a virus?
Several people have expressed very sweeping criticisms of virology as a discipline. For example, twenty doctors and investigators recently published a memorandum entitled “Settling the Virus Debate” [9]. In it, we read:
Further on, the authors make it clear that they don’t agree with the use of cell cultures as part of the isolation procedure. According to them, cell cultures may on their own give rise to debris that might be mistaken for virus particles, and they therefore insist that a virus must be directly isolated from tissues or bodily fluids of infected humans or animals. This objection can be countered as follows:
- The particles of many viruses have very characteristic shapes that are not likely to be confused with any particles produced by living cells, or with debris left behind by dead cells.
- There are many biochemical methods for characterizing viral particles, and moreover for establishing that they contain genetic information characteristic of the virus rather than the host cell culture.
- Not all viruses can easily be grown in cell cultures. Those which cannot are indeed routinely propagated in, and directly isolated from, laboratory animals.
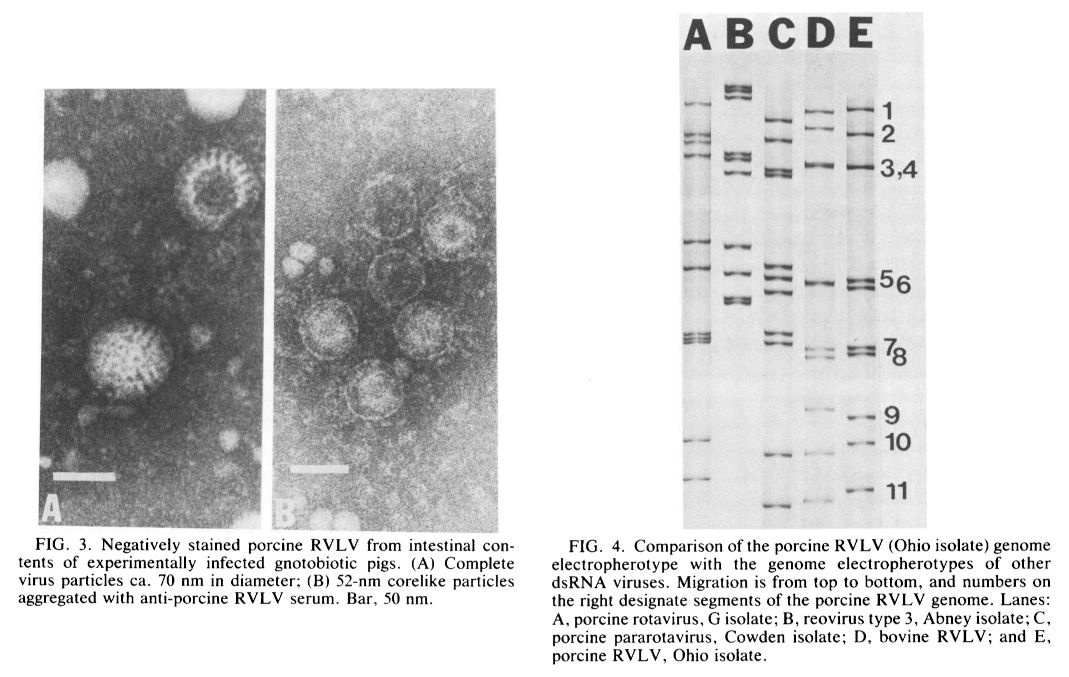
A good example of such an animal study was published by Theil et al. [10]. It concerned the isolation of a novel virus from gnotobiotic, i.e. otherwise germ-free pigs. The abstract of the study reads as follows:
The study shows both electron-microscopic pictures of the viral particles, as well as the result of an electrophoresis experiment that compares the genetic material contained in these particles to those of known viruses with similar morphology (see Figure 2). The novel virus could be serially passaged through multiple pigs without becoming “diluted” or getting lost altogether; therefore, it was clearly replicating within those pigs. Infection was detectable in the intestinal cells of the pigs and gave rise to diarrhea. We can see no reasonable objection to the authors’ conclusion that they had in fact established the existence of a novel virus that causes intestinal disease in pigs.
While direct isolation is often used in the initial characterization of a novel virus, the use of cell cultures greatly facilitates the sensitive and speedy routine detection of viruses that are already known. It is unrealistic to expect that practicing virologists will forgo the use of this expedient just to accommodate the radical armchair skeptics. It is not reasonable to blame virologists for going about their job in the most efficient manner.
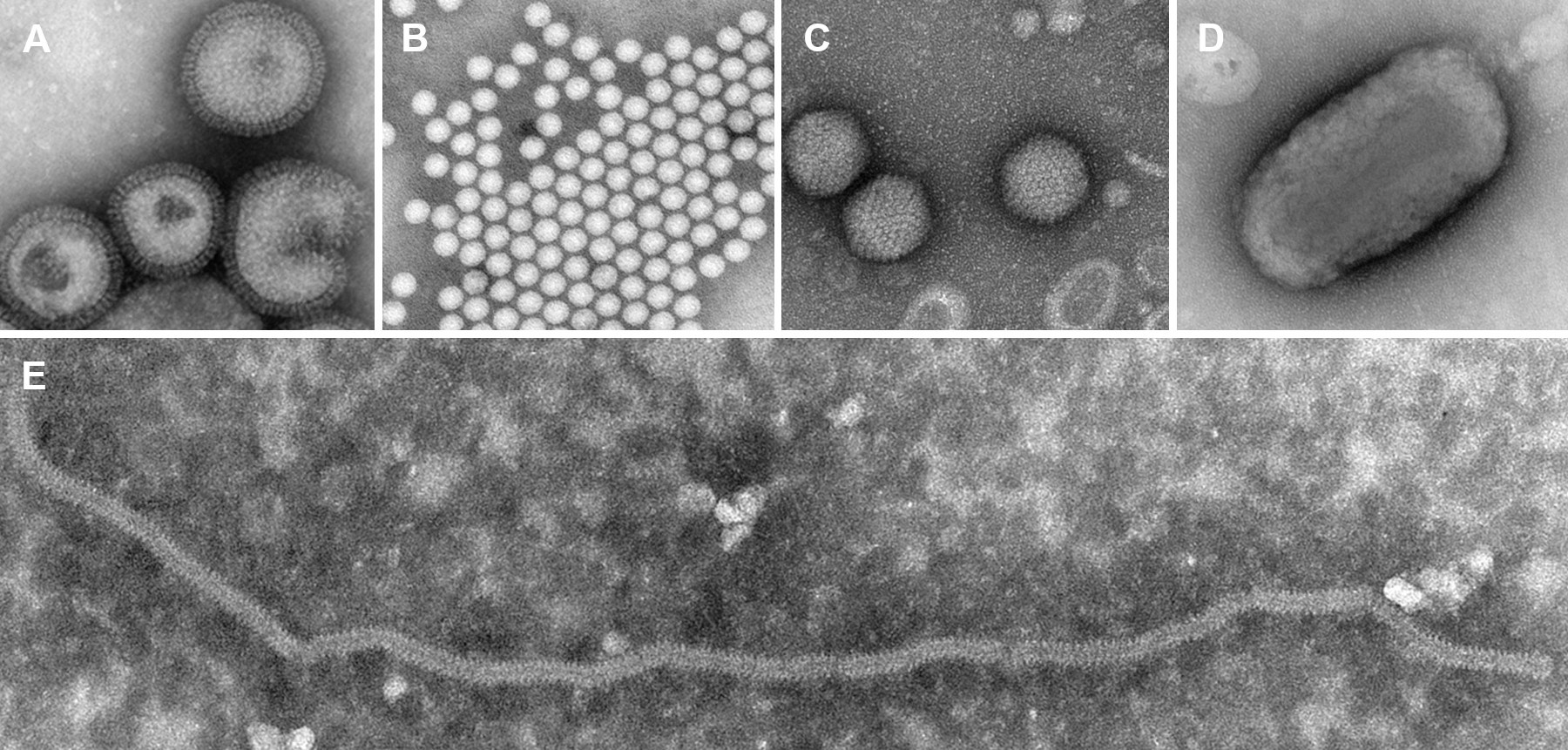
6. Viruses are diverse
Virus particles differ considerably in size and shape. This is illustrated in Figure 3. The electropherogram shown in Figure 2 illustrates that even viruses with similar morphology can be distinguished from one another using biochemical methods. Nowadays it has become commonplace to determine the nucleotide sequences of virus isolates, which gives an even more fine-grained differentiation. Of note, the artificial nature of SARS-CoV-2 can be convincingly demonstrated based on nothing more than the nucleotide sequence of its genome [11].
The very first electron-microscopic image of a virus—in the specific case, the tobacco mosaic virus, which infects tobacco plants—was acquired in 1939, by a team of researchers that included Helmut Ruska, the inventor of the electron microscope [13]. But even two years earlier, Thomas Rivers had every reason to write, in his essay “Viruses and Koch’s postulates” [14]:
Even without any of these structural and biochemical distinctions, the diversity of viruses is already clear from clinical observations alone. No physician or nurse will confuse poliomyelitis with smallpox or yellow fever with measles. Likewise, no virologist will mistake the causative viruses of these diseases for one another. Viruses have a plethora of well-defined properties that distinguish them unambiguously from one another, as well as from any and all particles released by living or dying cells that are not virus-infected.
7. Has the SARS-CoV-2 virus ever been isolated?
Yes, it has been—numerous times. An overview of such studies has been provided by Jefferson et al. [15]. A solid study that correlates virus isolation, PCR and clinical findings in a series of hospitalized COVID-19-patients has been published by Wölfel et al. [16]. It is also possible to buy samples of the purified virus from the American Type Culture Collection. These are heat-inactivated, but they should still permit investigators with the required expertise and equipment to confirm the identity of the virus.
The legend that SARS-CoV-2 has never been isolated is founded solely on the rigid demand that such isolation be accomplished without the use of cell cultures. As noted before, practicing virologists are highly likely to ignore this demand, for which we cannot fault them.
8. But isn’t COVID-19 just the flu rebranded?
It was indeed quite striking that concomitantly with the rise of COVID-19 case numbers those of influenza took a nosedive. This can be understood as follows:
- It is quite common for respiratory infections to be caused by more than one virus. If testing is not comprehensive, then the tests chosen will skew the results.
- The hysteria around COVID-19 caused physicians to carry out diagnostic tests selectively for COVID-19, to the exclusion of other respiratory pathogens.
- Extremely loose criteria were used for diagnosing COVID-19 infections. You have likely heard of the widespread problems with false-positive PCR tests.
The flawed laboratory methods could not but lead to many spurious diagnoses of COVID-19. The patients so diagnosed were then usually not tested any further for influenza, which caused the number of diagnosed influenza cases to drop off. Failure to test for bacterial pathogens caused patients with bacterial pneumonia to go unrecognized and be denied the necessary treatment with antibiotics. This was just one of the many forms of medical malpractice in the COVID-19 era that were the real drivers of excess mortality [17,18].
Conclusion
While we have every reason to distrust and indict today’s medical and scientific establishment, this should not lead us to disregard solid scientific evidence where it exists. Germ theory in general and also virology are very rich in such evidence, notwithstanding their recent distortions and abuses, which must urgently be identified and corrected. However, the remedy lies not in radical skepticism bordering on nihilism. Instead, we must recapture and rekindle the spirit of rigorous but unprejudiced debate that once made medical science great.
Notes
- Today, Budapest’s medical university bears Semmelweis’s name. (go back)
References
- (2015) Skeptical of medical science reports?. Can. Vet. J. 56:1011-2
- (2005) Why Most Published Research Findings Are False. PLoS Med. 2:e124
- (2012) Not Even Trying: the corruption of real science (University of Buckingham Press).
- (2021) The Prevailing Corona Nonsense Narrative, Debunked in 10 or 26 Minutes.
- (1982) `Über Tuberkulose.’ A tribute to Robert Koch’s discovery of the tubercle bacillus, 1882. Tubercle 63:3-17
- (2020) The Cholera Epidemics in Hamburg and What to Learn for COVID-19 (SARS-CoV-2). Cytometry A 97:337-339
- (1915) Rural sanitation in the tropics (John Murray).
- (2024) History of tuberculosis.
- (2022) Settling the Virus Debate.
- (1985) Porcine rotavirus-like virus (group B rotavirus): characterization and pathogenicity for gnotobiotic pigs. Journal of clinical microbiology 21:340-5
- (2020) Unusual Features of the SARS-CoV-2 Genome Suggesting Sophisticated Laboratory Modification Rather Than Natural Evolution and Delineation of Its Probable Synthetic Route. Preprint DOI:10.5281/zenodo.4028830
- (2009) Modern uses of electron microscopy for detection of viruses. Clin. Microbiol. Rev. 22:552-63
- (1939) Die Sichtbarmachung von pflanzlichem Virus im Übermikroskop. Naturwissenschaften 27:292-299
- (1937) Viruses and Koch’s Postulates. J. Bacteriol. 33:1-12
- (2020) Viral cultures for COVID-19 infectivity assessment. Systematic review. Clin. Infect. Dis. ciaa1764
- (2020) Virological assessment of hospitalized patients with COVID-2019. Nature 581:465-469
- (2021) Nature of the COVID-era public health disaster in the USA, from all-cause mortality and socio-geo-economicand climatic data.
- (2022) COVID-Period Mass Vaccination Campaign and Public Health Disaster in the USA. ResearchGate DOI:10.13140/RG.2.2.12688.28164
