Michael Palmer, MD
This short memo makes the case that turbo cancers in patients who received mRNA vaccines can be explained by the observed uptake of those vaccines by macrophages and dendritic cells, based on a well-documented but not widely known theory of carcinogenesis.
An increasing number of clinical oncologists and pathologists are reporting cases of solid cancers, lymphomas and leukemias which stand out to them due to their unusually rapid growth and progression to systemic metastasis, and which have began to appear some time after the roll-out of the mRNA vaccines against COVID-19. To my knowledge, no precise explanation has yet emerged to account for this unusual behavior.
Most doctors and cancer researchers consider DNA damage the primary cause of malignancy; and it is true that the mRNA vaccines can potentially induce genetic damage in a variety of ways:
- the cationic lipids contained in them will promote the formation of reactive oxygen species, which will chemically damage the cellular DNA;
- the contamination of these vaccines with plasmid DNA fragments implies a risk of insertional mutagenesis;
- the mRNA itself may be reversely transcribed into DNA, which will then also insert into the chromosomal DNA; and
- a study that was retracted for somewhat opaque reasons has documented the inhibition of DNA repair by the recombinantly expressed spike protein.
However, while such vaccine-induced DNA damage might explain an increased risk of cancer in principle, it does not seem to account for the unusually rapid and aggressive growth of these cancers. We therefore should seriously look at different explanations, even different paradigms of carcinogenesis.
At a recent meeting near Stockholm, I was fortunate to get to know Dewey Weaver, an American entrepreneur who champions the idea of cancer being a primarily metabolic disease, and of devising treatments accordingly. Our conversation led me to the remarkable book “Cancer as a Metabolic Disease” [1] by Thomas Seyfried, a cancer researcher at Boston College. Seyfried’s hypothesis has two key elements:
- The primary event in carcinogenesis is an insult to the mitochondria, which disrupts the respiratory chain in this organelle. This is essentially the same idea which Otto Warburg published almost 100 years ago, but Seyfried adds some important detail to it, which reconciles this hypothesis with some apparently contrary evidence.
- Metastasis arises if cells of a cancer that so far has been only locally invasive fuse with macrophages or dendritic cells. The job description of macrophages and dendritic cells requires them to move about freely, entering and leaving the circulation at will—a behavior which metastatic cancer cells share with them. When a macrophage or dendritic cell fuses with a cancer cell whose pre-existing metabolic injury confers the trait of unrestricted growth, then all the traits required for metastatic cancer will be united in that fused cell.
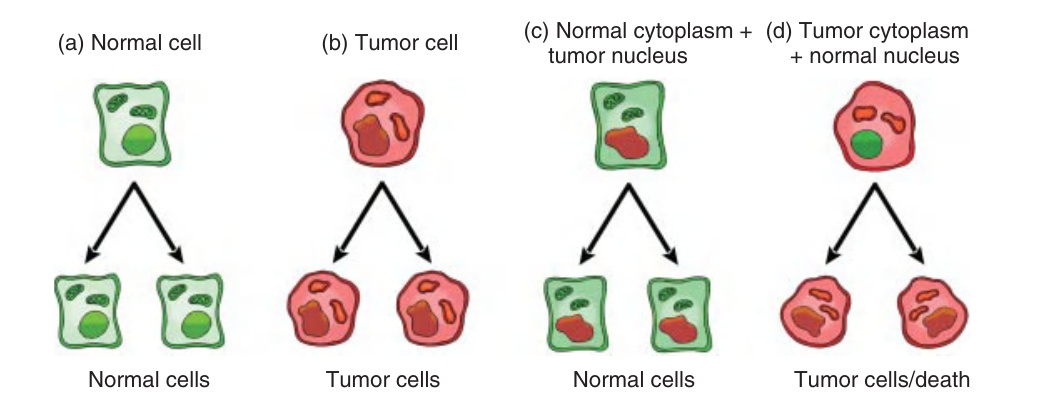
While I cannot possibly do justice to Seyfried’s work here, I will give just one bit of evidence—or more of a “teaser,” really—from his book. Figure 1, and the accompanying caption, have been lifted from his Fig. 11.3. They summarize a number of experimental studies conducted independently by various labs, and which clearly show that, if one separates the nucleus from the cytoplasm of a cancer cell, the trait of malignancy travels with the cytoplasm, not the nucleus.
To anyone still able to think straight after all these years of crazy fake “science,” this signifies to the genetic theory of cancer the same as the Michelson-Morley experiment did to the ether and the absolute coordinate system of the universe—namely, the tree at the sudden bend of the road. It is true that experiments of this kind do not specifically implicate the mitochondria; but for multiple reasons also laid out by Seyfried, these must indeed be considered the leading candidate.
How, then, does Seyfried’s theory tie in with the causation of turbo cancer after vaccination?
In connection with the COVID-19 vaccines, we have been told that their main purpose was to induce antibodies, even though this is a rather futile approach for immunizing against a respiratory pathogen. Efficient antibody formation requires the activation of antigen-presenting cells, in particular dendritic cells, macrophages, and B-lymphocytes; and indeed one can easily find articles that highlight the ability of the mRNA-lipid nanoparticles to make their way to such antigen-presenting cells. Pathologists Arne Burkhardt and Walter Lang found spike protein-expressing dendritic cells and macrophages in some of their tissue specimens from living and dead vaccine victims.
One of the biological functions of the SARS-CoV-2 spike protein is to bring about the fusion between the viral envelope and the membrane (either cytoplasmic or endosomal) of the target cell. The surface proteins of other enveloped viruses share that function. If such proteins begin to appear on the surface of an infected cell, then this may cause that cell to fuse with neighboring cells. Such fused “giant cells” or syncytia are very commonly observed with measles, and in the case of the Respiratory Syncytial Virus this phenomenon is reflected even in the name. Thus, it is reasonable to expect that dendritic cells and macrophages expressing spike protein will have an increased tendency to fuse with other body cells.
That leaves the question of mitochondrial injury, which confers the trait of unlimited growth. In cancer that is not vaccine-related, this trait will probably be conferred in most cases by cells from the locally invasive cancer that is turned into a metastatic one through fusion with macrophages. This may also often be the case in vaccine-associated turbo cancer; then, some local, small and as yet undetected cancer will indeed be “turbo-charged” by fusion with a vaccine-primed macrophage.
However, we must also consider the possibility that the vaccine-primed macrophage will confer both the fusion activity and the mitochondrial injury, the latter having been caused by the chemical toxicity of the lipid nanoparticles; the above-mentioned induction of reactive oxygen species arises at least in part from disrupted mitochondrial respiration. In that case, one might expect some such cells to turn into metastatic malignancies all by themselves. I am not familiar enough with the cancer cases currently being observed to decide whether or not this fits the evidence.
One more word about lymphomas, which according to several experts figure quite prominently among the turbo cancers. Lymphocytes, too, travel quite freely between various tissues and the circulation, and it might be that they do not need to fuse with macrophages in order to become malignant. Spike protein has been detected by immunohistochemistry in lymphocytes, too, and in their case the concomitant mitochondrial injury might already suffice to turn them into malignant lymphomas.
If this hypothesis were broadly true, where would this leave us? Some conclusions are:
- the theory of carcinogenesis by injury to mitochondrial metabolism and metastasis by macrophage fusion scores where the genetic theory of cancer does not;
- it is urgent that we begin to take the metabolic theory of carcinogenesis seriously, and that we follow the leads it gives us for cancer treatments.
In this connection, we must remember another observation by those aforementioned oncologists—namely, that “turbo cancers” show very poor response to the conventional cytotoxic cancer chemotherapy.
I apologize for writing this memo in haste and not properly referencing it—but most of the recipients will probably know most of the studies which I have alluded to. I will hopefully get around to writing an enhanced version soon, but I felt the urge to share it even in this preliminary form.
References
- (2012) Cancer as a Metabolic Disease (John Wiley & Sons).
