Michael Palmer, MD
This paper summarizes the mode of action of mRNA vaccines, as well as three potential pathogenetic mechanisms that may account for the toxicity observed with the mRNA vaccines against COVID-19, namely: chemical toxicity of lipid nanoparticles, direct toxicity of the spike protein, whose expression is induced by the vaccines, and the destructive effects of the immune response to the spike protein. The case is made that of these mechanism the third is likely the most important one. If this conclusion is correct, then essentially the same level of toxicity must be expected with future mRNA vaccines against any other pathogenic microbes.

1. How mRNA vaccines provoke immune attack on our own cells and tissues
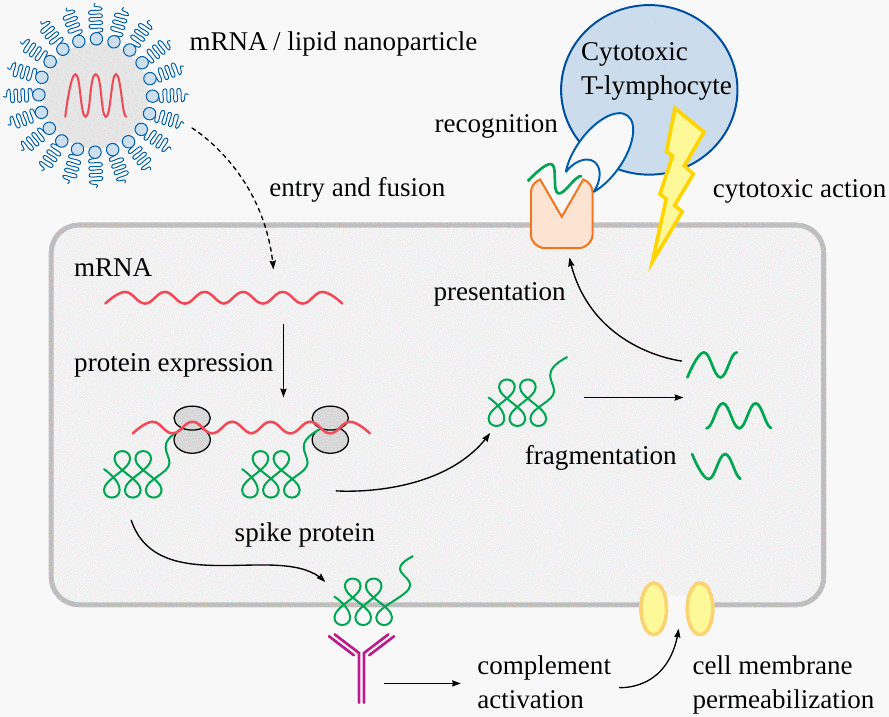
mRNA vaccine particles have two components—the mRNA itself, and the lipid mixture which encloses it. The lipids protect the mRNA while in transit, and they facilitate its cellular uptake.
Once within the cell, the mRNA binds to ribosomes—the little grey blobs in the cartoon—which read the sequence of the mRNA and assemble the protein accordingly. In case of the COVID-19 vaccines, the product is the spike protein of the SARS-CoV-2 virus.
The spike protein will be taken to the cell surface, where it may be bound by antibodies. Those bound antibodies will activate the complement system, a cascade of serum proteins which culminates in the formation of a membrane attack complex. Such complexes create large holes in the cell membrane, ultimately killing the cell.
Another pathway to immune attack begins with the fragmentation of some spike protein molecules within the cell. The fragments are again taken to the cell surface, where they are recognized by cytotoxic T-lymphocytes (T-killer cells). Recognition causes them to attack and kill the infected cell.
The above assumes that we already have antibodies which recognize the spike protein or its fragments. How do these arise in the first place? Without going into details, we note that their induction requires some measure of cell damage and cell death, brought on for example by T-killer cells. The antibody response is then induced by the debris of those dead cells.
1.1. Sure, that looks pretty bad, but aren’t mRNA vaccines just like live virus vaccines?
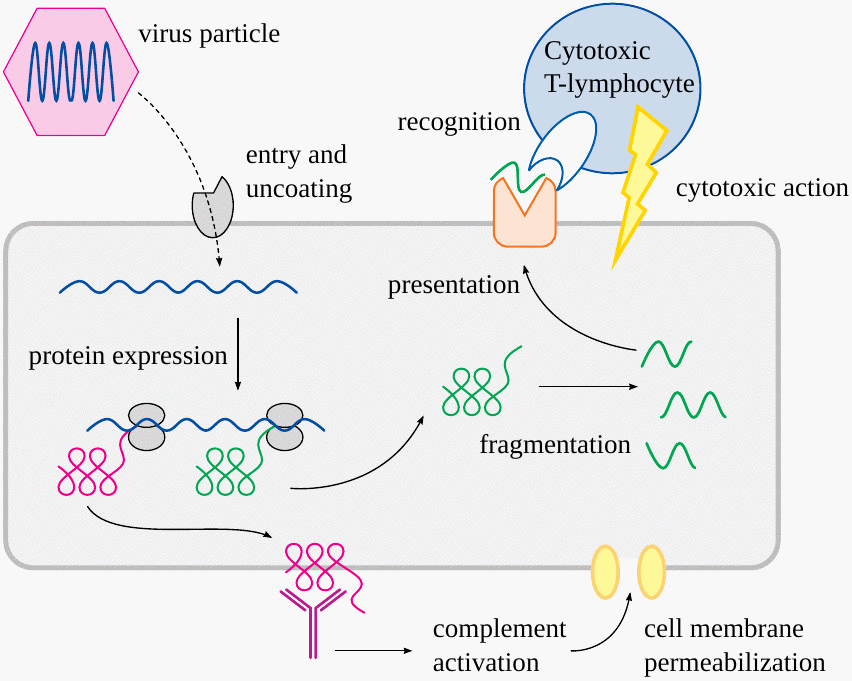
It is true that the same two pathways also operate in the immune defence against natural viruses and live virus vaccines. However, the devil is in the details.
1.2. Three key differences between live virus vaccines and mRNA vaccines
| Live virus vaccines | mRNA vaccines | |
| Replication inside the host cell | yes | no |
| Vaccine particles contain protein antigens | yes | no |
| Vaccine particles infect blood vessel walls | no | yes |
We will see presently why these three differences are important.
1.3. The time course of viral load and immune response in a virus infection or live virus vaccination
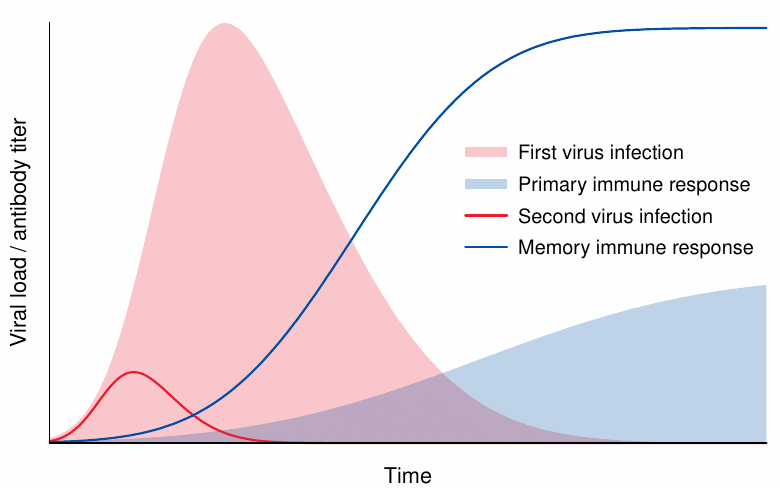
If we are infected with a natural virus or inoculated with a live virus vaccine, the initial viral load is small. In the absence of prior immunity, the virus will replicate for a good while, and the viral load will increase until it is checked by the onset of the immune response. By the time the immune response reaches its peak, the viral load will typically already have declined, and the fight against the infection will be at the “mop-up” stage.
A secondary infection will trigger a memory response, which curbs the multiplication of the virus early on. Therefore, the peak of the viral load will remain much lower, and the infection will often not even be clinically apparent—we are “immune” to it. Again, any small-scale infection that does occur will be largely gone by the time the immune response attains its peak. Thus, neither with the primary infection nor with a secondary one will peak viral load and peak immune response clash head-on. This limits the intensity of inflammation.
1.4. Repeat injections of mRNA vaccines will clash with existing immunity
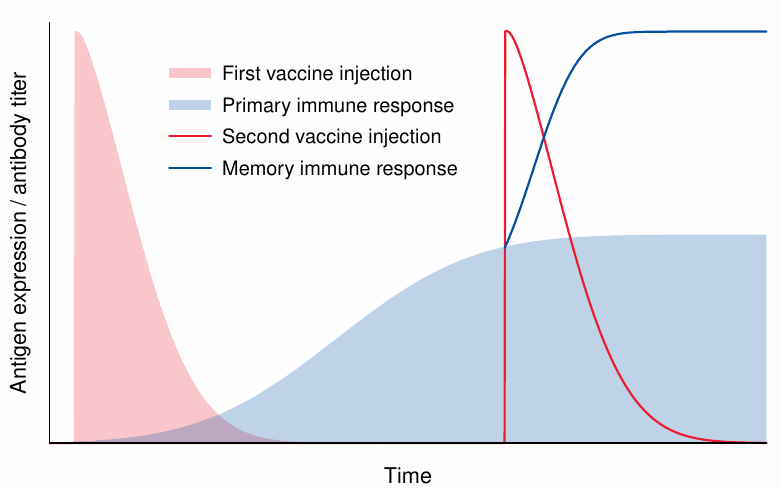
We now come to the first disparity between viruses and mRNA vaccines—namely, that unlike viruses mRNA vaccines do not replicate. This makes it necessary to inject the full amount of vaccine particles all at once and every time.
The expression of the antigen is supposed to decline on a time scale of days. If we assume this to be the case, and also that no immunity yet exists, we may again avoid a clash between peak antigen expression and peak immune response. However, with a repeat injection, and also in case of natural immunity due to a previous infection with the virus, we must expect antigen expression to clash head-on with an intense immune response, resulting in accordingly intense inflammation. Thus, both acute side effects and long-term ones such as autoimmune disorders will become more likely after the second shot.
1.5. Unlike viruses, mRNA vaccine particles aren’t recognized by antibodies
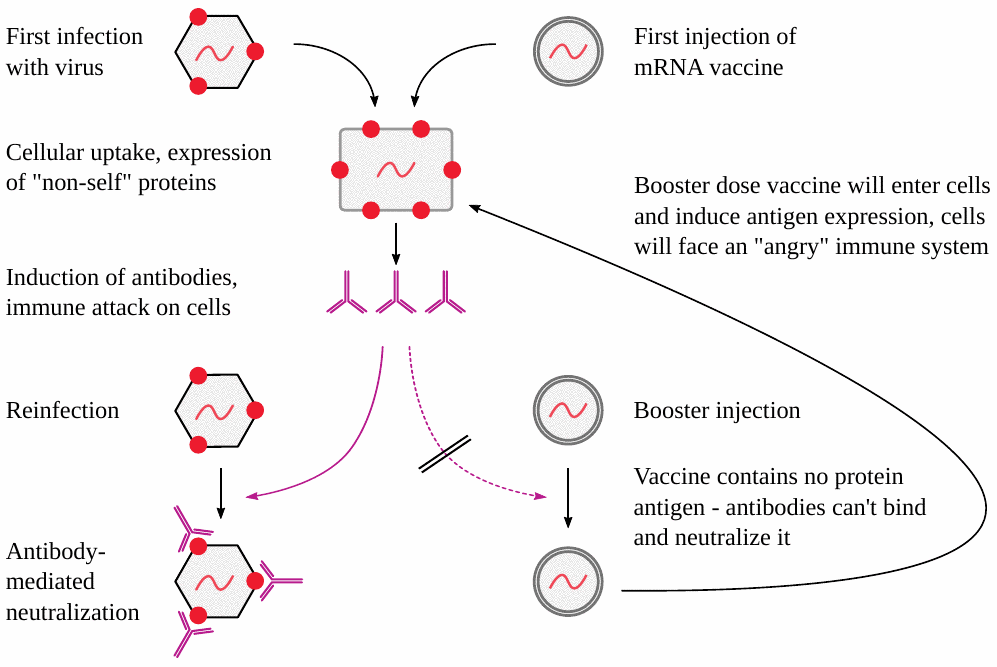
The concern about the head-on clash between vaccine antigen expression and immune response is compounded by the second disparity between viruses and mRNA vaccines—namely, that the mRNA vaccine particles do not contain any copies of the encoded protein antigen on their surfaces.
The presence of protein antigens on virus particles means that these can be bound by antibodies that are already present, which will prevent those virus particles from infecting our body cells. Even though some particles may still manage to get through, the antibodies will at least mitigate the infection.
In contrast, mRNA vaccine particles cannot be stopped by antibodies at all, for the simple reason that they contain only the nucleic acid blueprint for the protein but not the actual protein itself. Therefore, these particles will be taken up by our body cells regardless of immunity. Any immunity already present will then be directed against those unlucky cells.
Thus, in a nutshell, with real viruses existing immunity will inhibit cell damage and inflammation, while with mRNA vaccines existing immunity will make things worse.
1.6. Summary: the inherent flaws of mRNA vaccines
- High particle load clashes with intense immune response
- Particles “fly under the radar” of antibody surveillance before entering cells, directing an “angry” immune system against those cells
- Antigen expression in cells of blood vessel walls causes destruction of vessels, with activation of blood clotting
The first two points promote intense inflammation, with severe tissue destruction and the risk of triggering autoimmunity. Damage to blood vessels poses grave risks as well; this is illustrated by the severe disease caused by those natural viruses which do infect blood vessel walls. Examples are the Ebola, Marburg, and Dengue viruses.
2. Adverse event severity after repeated vaccine injection
2.1. Increased severity of adverse events in teens after the second shot of Moderna vaccine
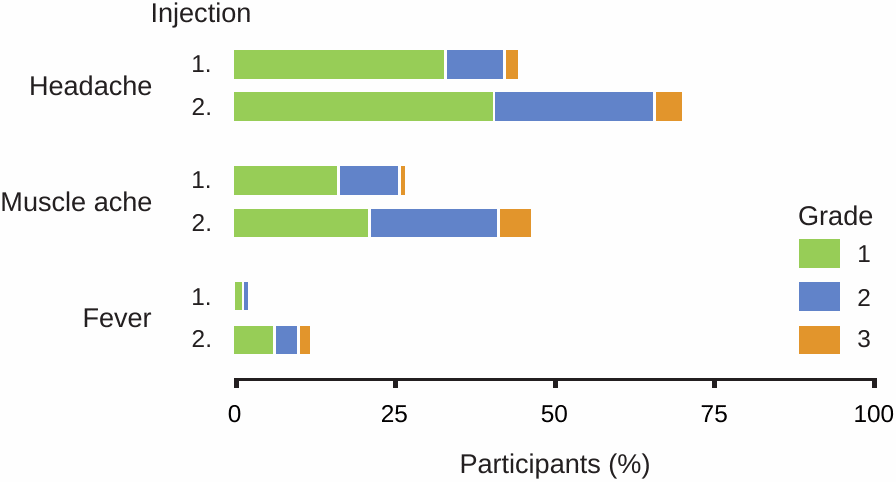
This figure is adapted from Ali et al. [1], the “clinical trial” on the Moderna vaccine in teenagers. We see a general increase in severity after the second injection, particularly with grade 2 and 3 side effects. Grade 3 fever means between 39 and 40 degrees centigrade. Such high fever signals a potential for severe inflammation and is normally considered unacceptable in a vaccine candidate.
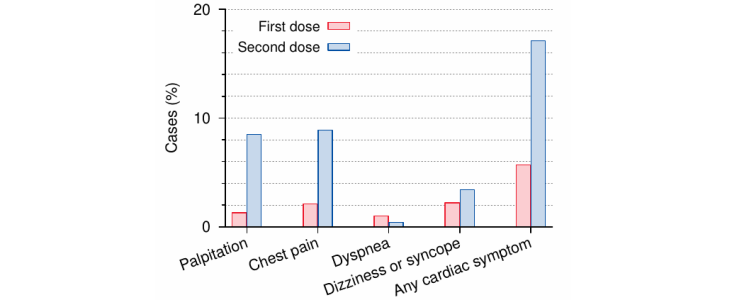
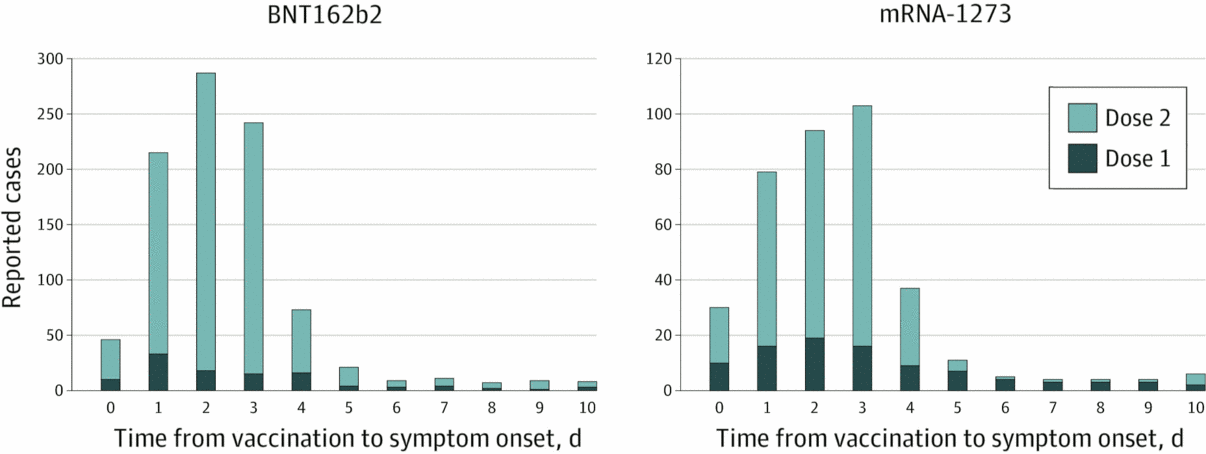
2.2. Cardiac symptoms in teens after first and second injections with the Pfizer vaccine
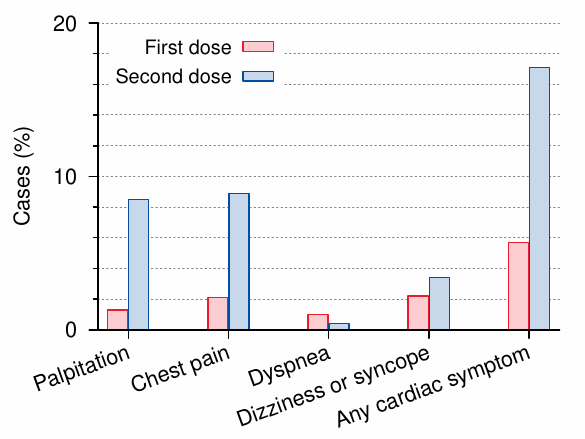
The data in this figure are from Chiu et al. [2], who followed approximately 5000 injected teenagers. We see a clearly increased incidence of symptoms after the second injection.
The cardiac symptoms monitored in this study are comparatively “mild”, but they are very frequent, leading us to expect that more severe cardiac consequences will occur as well. Many of these symptomatic vaccinees likely incurred some degree of inflammation in the heart.
2.3. VAERS reports of myocarditis after the first and the second dose
Of course, we already know that vaccine-induced myocarditis is not rare. This figure (adapted from Oster et al. [3]) shows that with myocarditis, too, the incidence is significantly higher after the second injection than the first. A study from Basel in Switzerland suggests an even higher incidence after the third injection [4].
2.4. Days to death by age and dose (VAERS, up to 2021-11-23)
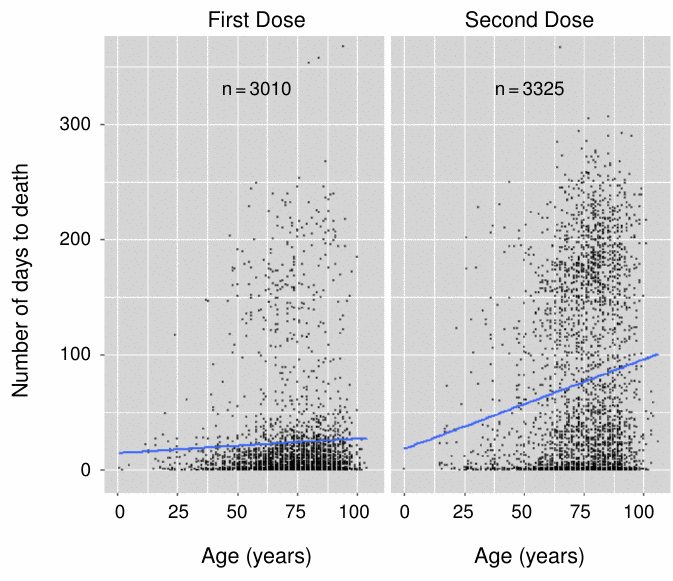
This analysis, carried out by Craig Pardekooper of “How bad is my batch” fame [5], suggests that the story is a little more complicated. Apparently, there are more delayed deaths, but fewer early ones after the second dose.
The total numbers of deaths in both panels are quite similar. However, it stands to reason that the likelihood of the connection being made between an injection and a death or other severe adverse event decreases with time; or in other words, that the under-reporting bias will increase with time. Therefore, delayed deaths are likely under-represented relative to the early ones. This suggests that overall mortality will be significantly greater after the second dose.
3. Alternate mechanisms of vaccine injury
- Chemical toxicity of lipid nanoparticles
- Spike protein toxicity
- Immune response to spike protein as a foreign antigen
- Induction of genetic mutations by the mRNA and by contaminating DNA
In the following, we will look briefly at the first three mechanisms, and then consider which one is most likely predominant. The fourth mechanism was discussed in a previous article [6].
3.1. Cationic lipids are highly inflammatory

This figure is adapted from a paper by Ndeupen et al. [7], who injected mice with lipid mixtures similar to those used in the COVID-19 mRNA vaccines. The left panel shows excised skin patches from mice that had been injected with buffer (PBS) only, with an inert lipid mixture (nNLP), or with a lipid mixture containing cationic lipids (iLNP). In the latter case, the skin patches are bloodshot, indicating inflammation. The plots to the right show that inflammatory cells, in particular neutrophil granulocytes, are increased in this case as well.
3.2. Cationic lipids induce reactive oxygen species, which can induce apoptosis (programmed cell death)

Cationic lipids can also induce programmed cell death (apoptosis), which can be detected by DNA fragmentation, as shown in this electrophoresis experiment. DNA fragments are here separated according to size—the further from the origin on the left, the smaller they are. In cell cultures, this effect can be suppressed by the addition of a reducing agent (N-acetylcysteine), which indicates that it is mediated by reactive oxygen species (ROS).
The induction of ROS by cationic lipids has been confirmed in multiple studies, and it poses a risk of DNA damage even if the threshold of outright apoptosis is not reached. This risk is further substantiated by some very fragmentary data on genetic damage in red blood cell precursors, which were submitted by Moderna to the European Medicines Agency [8].
3.3. Toxic activities of spike protein
- Spike protein fragment S1 can be cleaved off cell surfaces and enter the bloodstream
- S1 fragment binds and inhibits angiotensin converting enzyme (ACE2)
- ACE2’s substrate, angiotensin II, accumulates and causes
- elevated blood pressure
- activation of blood clotting
- increased inflammation
- Intracellular spike protein inhibits DNA repair
The spike protein itself also has toxic activity, which may be mediated by inhibition of ACE2 [9,10] and potentially also by the inhibition of DNA repair [11], which may compound the mutagenic risks posed by the RNA and contaminating DNA [6] as well as the cationic lipids.
3.4. Immune pathology after vaccination (“lymphocyte amok”)

This slide shows normal heart muscle tissue for comparison, and heart muscle tissue affected by vaccine-induced myocarditis, as evident from the cluster of lymphocytes in the middle. This image is from an autopsy case reported by pathologist Prof. Arne Burkhardt, who has used the term “lymphocyte amok” to sum up his findings in many organs and in many patients who had died after receiving gene-based COVID-19 vaccines.
3.5. Healthy lung tissue, and clusters of lymphocytes in the lung of a vaccine victim

This picture, likewise from Prof. Burkhardt, shows lymphocytic inflammation of the lung. The normally delicate alveolar septa of the lung tissue are thickened by scar tissue, and the air-filled spaces (white) are compressed.
The dark blue dots in the left panel are the cell nuclei of the regular cells within the tissue. Some of the blue dots in the right panel are of the same nature. However, the large cluster within the top left quadrant is an accumulation of invading lymphocytes.
3.6. Vasculitis of small blood vessels in the brain
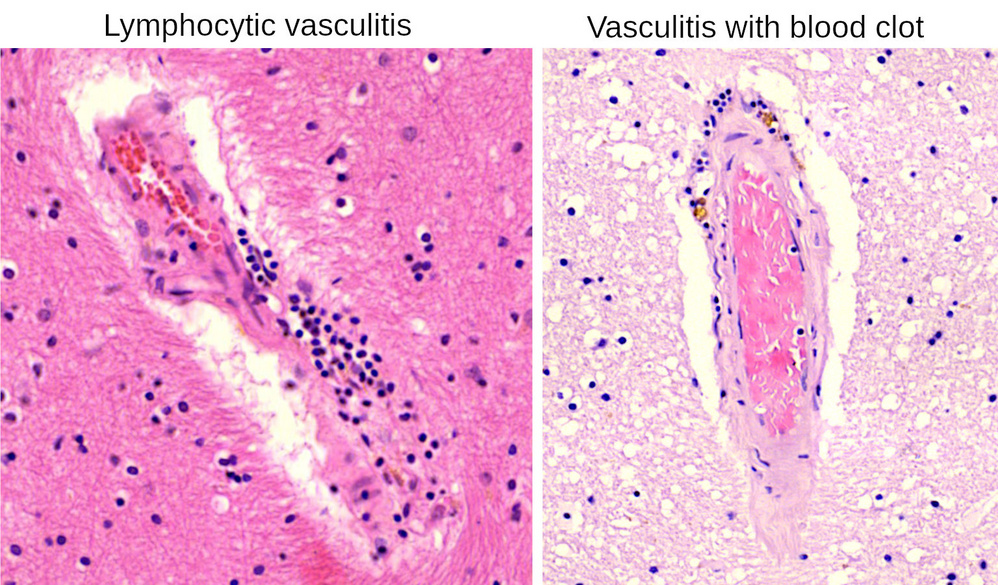
Blood vessels of all sizes are prominently affected by lymphocytic inflammation. This slide (again by Prof. Burkhardt) shows two inflamed small vessels within brain tissue. On the right, the inflammatory lesions have caused the blood within the vessel to clot.
Lymphocytes are also seen in the surrounding brain tissue itself, indicating that inflammation is not limited to the blood vessels.
3.7. Spike protein expression in a case of vaccine-induced encephalitis
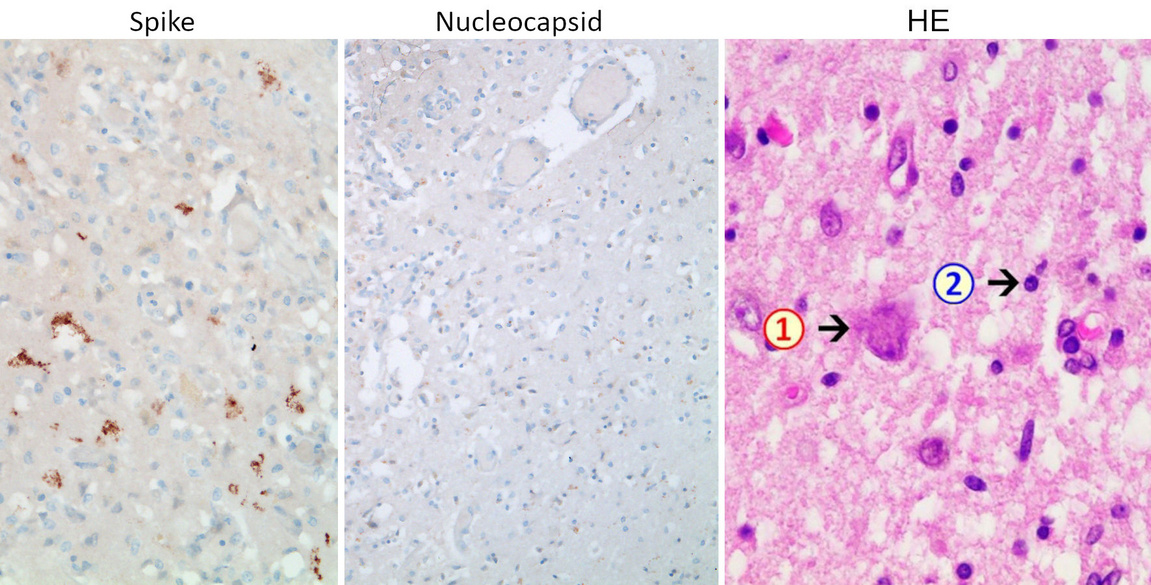
The causal connection between vaccine injection and inflammation can be demonstrated by immunohistochemistry. In this method, the specificity of antibodies for a given protein of interest—such as in our case the spike protein—is used for its sensitive and selective detection in tissue sections. Several steps downstream of antibody binding, a brown pigment is generated that shows the presence and distribution of the target protein.
This slide shows brain sections from a patient who died several weeks after receiving his most recent COVID-19 vaccine injection [12]. The conventional (HE) stain on the right shows a dead nerve cell (1) and inflammatory cells including lymphocytes (2). The diagnosis made was necrotizing encephalitis, i.e. brain inflammation with cell/tissue death.
In the left panel, we see that spike protein is expressed by several cells in a sample of brain tissue, as evidenced by the deposition of brown pigment atop those cells. The middle panel shows that the nucleocapsid—another protein of the SARS-CoV-2 virus—is not expressed. The vaccine encodes only the spike, whereas virus-infected cells should express all viral proteins, also including the nucleocapsid. Therefore, the spike protein which is detected must have been induced by the vaccine. This fits with the clinical history in this case, which included three vaccinations but no diagnosis of the virus infection.
3.8. Myocarditis with complement deposits and primarily granulocytic infiltrates
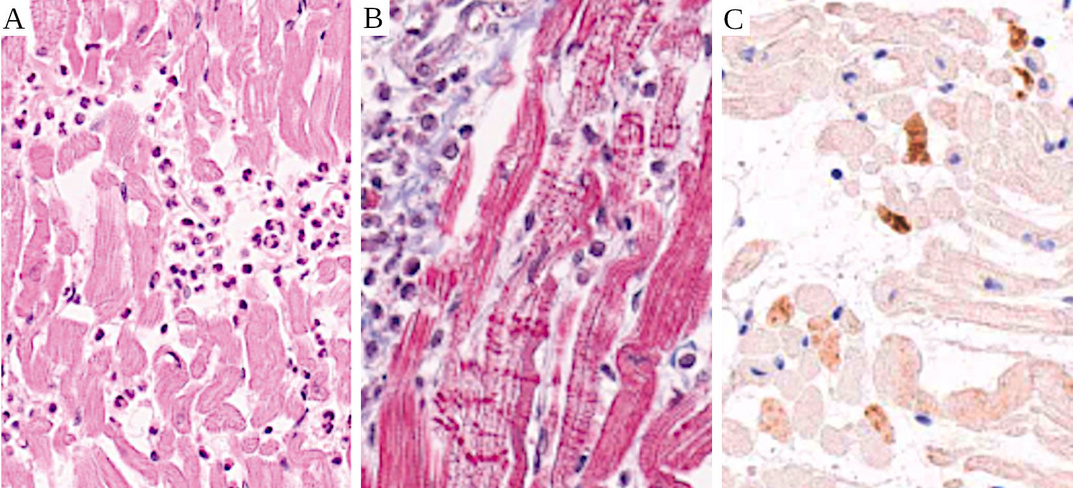
This case of myocarditis with sudden death was reported by Choi et al. [13]. Five days after the first dose of Pfizer vaccine, the patient developed chest pain, and he died seven hours later. Complement factor C4 deposits are shown by immunohistochemistry in panel C. Cellular infiltrates predominantly with neutrophil granulocytes are seen in panels A and B. The horizontal red stripes in panel B are contraction band necroses, which are known to occur after intracellular calcium excess.
Complement activation will result in membrane permeabilization (see Section 1), which accounts for the calcium excess and the contraction band necroses. Complement activation will also release chemotactic factors that will attract granulocytes to the scene. This case therefore exemplifies the antibody/complement-mediated pathway of immune attack on cells which express the mRNA vaccine-encoded antigen. Most likely, the unfortunate patient already had strong natural immunity to the SARS-CoV-2 virus.
4. Which of the three mechanisms is the dominant one?
| Mechanism | Expected effect of 2nd dose | Comment |
| Lipid toxicity | no change | toxicity of adenovirus-based vaccines? |
| Direct spike protein toxicity | reduced | responsible for rapid effects of first dose? |
| Immune response to spike protein | increased | completely general—must be expected with all future mRNA vaccines |
One key consideration for identifying the dominant mechanism of mRNA vaccine toxicity is how each of them should change in intensity with the second injection.
With the cationic lipids, one might expect similar levels of acute toxicity after each application, although some degree of cumulative acute toxicity is conceivable. We note, however, that the spectrum of adverse events observed with adenovirus-based COVID-19 vaccines is very similar to that of the mRNA vaccines, even though the virus-based vaccines don’t contain any cationic lipids. This finding suggests that the common toxic principle of both vaccine types is the spike protein—either its direct toxicity, or the immune response to it.
Direct spike protein toxicity should be mitigated by specific antibodies to it, just as diphtheria and tetanus are mitigated by antibodies to their respective protein toxins. Thus, we should expect that the antibodies induced by the first vaccine injection should reduce the severity of adverse events that follow the second injection. However, as noted in Section 2, the severity of side effects tends to increase with repeated application of the vaccine. The one exception were early deaths, which were indeed more frequent after the first injection than the second one (see Section 2.4). The same trend was also found by Craig Pardekooper with non-deadly adverse events. It seems possible, therefore, that many adverse events which occur early on after the first injection are indeed related to the direct toxicity of spike protein, which manifests itself in the time window between the injection and the induction of antibodies.
A key role of the immune response to spike protein is supported by the following arguments:
- it follows from the theoretical considerations spelled out in Section 1;
- it agrees with the predominant trend of increased adverse event incidence and severity after repeated vaccine injection;
- it accounts for the histopathological findings of intense inflammation and infiltration with lymphocytes as well as other immune cells, which are observed near foci of spike protein expression.
Why does it matter which of the pathogenetic mechanisms is predominant? There are plans to convert existing vaccines, including childhood vaccines, to mRNA technology. If direct toxicity of the SARS-CoV-2 spike protein were mainly responsible for the adverse events caused by the COVID-19 mRNA vaccines, then future mRNA vaccines might be more benign, as long as the antigenic proteins which they encode are less toxic than the SARS-CoV-2 spike protein.
On the other hand, every mRNA vaccine will induce an immune response in the same manner as the COVID-19 mRNA vaccines. Therefore, if that immune response were mainly responsible for toxicity, then we must expect similarly catastrophic outcomes with all future mRNA vaccines. The arguments presented in this study indicate that this is the most likely case.
The contributions of the other two mechanisms cannot be ignored. Direct toxicity appears to significantly contribute to early toxicity after the first injection. Cationic lipid toxicity cannot be dismissed either, for the following reasons:
- almost no safety studies were conducted on these substances during the dysfunctional approval processes of the COVID-19 vaccines, but the rudimentary ones which were performed gave clear indications of toxicity;
- the induction of reactive oxygen species (ROS) by cationic lipids will cause DNA damage. This damage will stay behind even after the lipids themselves have been eliminated, which means that toxicity will be cumulative;
- since cationic lipids are a necessary ingredient of all mRNA vaccines, their toxicity will accumulate across all doses of all mRNA vaccines, rather than just across all doses of a single one.
In conclusion, the whole of the evidence indicates that all three mechanisms of toxicity must be taken seriously. At the same time, it points to a key role of immune-mediated toxicity, which results from the fundamental flaws of the mRNA vaccine technology and must be expected to occur with future mRNA vaccines directed against any and all viruses or other pathogenic microbes.
References
- (2021) Evaluation of mRNA-1273 SARS-CoV-2 Vaccine in Adolescents. N. Engl. J. Med. DOI:10.1056/NEJMoa2109522
- (2023) Changes of ECG parameters after BNT162b2 vaccine in the senior high school students. Eur. J. Pediatr. 182:1155-1162
- (2022) Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021. JAMA 327:331-340
- (2022) Significant incidence of myocarditis after 3rd dose of RNA vaccine anti-COVID messenger 19.
- (2023) How Bad is My Batch? Batch codes and associated deaths, disabilities and illnesses for Covid 19 Vaccines.
- (2023) COVID-19 mRNA vaccines contain excessive quantities of bacterial DNA: evidence and implications.
- (2021) The mRNA-LNP platform’s lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory. iScience 24:103479
- (2021) EMA Assessment report: COVID-19 Vaccine Moderna.
- (2021) An overview of the MATH+, I-MASK+ and I-RECOVER Protocols (A Guide to the Management of COVID-19).
- (2022) COVID-19, vaccines and deficiency of ACE2 and other angiotensinases. Closing the loop on the “Spike effect”. Eur. J. Intern. Med. 103:23-28
- (2021) SARS-CoV-2 Spike Impairs DNA Damage Repair and Inhibits V(D)J Recombination In Vitro. Viruses 13:2056
- (2022) A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against Covid-19. Vaccines 10:2022060308
- (2021) Myocarditis-induced Sudden Death after BNT162b2 mRNA COVID-19 Vaccination in Korea: Case Report Focusing on Histopathological Findings. J. Korean Med. Sci. 36:e286